![]() It’s the injury we see most often as coaches and something we always acutely aware of as runners.
It’s the injury we see most often as coaches and something we always acutely aware of as runners.
Iliotibial band syndrome (ITBS) is the second leading cause of knee pain in runners and is the number one cause of lateral knee pain. (1)
ITBS is an overuse running injury that results from repetitive friction of the IT band over the outside of the knee joint, with biomechanical studies demonstrating a maximal zone of impingement at approximately 30 degrees of knee flexion which occurs soon after heel strike when running.
Training factors related to this injury include excessive running in the same direction on a track, greater-than-normal weekly mileage and downhill running (2)
ITBS is a is related to a weak hip abductors
Long distance runners with ITBS have weaker hip abduction strength
in the affected leg compared with their unaffected leg and unaffected long-distance runners. Additionally, symptom improvement with a successful return to the preinjury training program parallels improvement in hip abductor strength. (3)
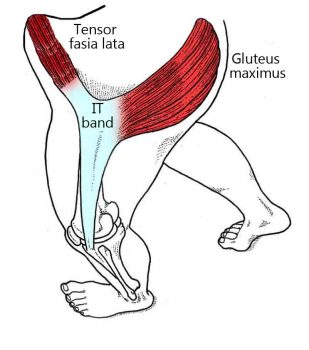
Hip abductor muscles include the gluteus medius, gluteus minimus, and tensor fascia lata (TFL)
Runners with ITBS exhibit significantly weaker hip abductor muscle strength in the affected limb compared to the non-injured limb and compared to the healthy runners. (4)
Strength work reduces prevalence ITBS
Large scale meta Analysis of almost 3500 separate studies indicate that “consistently favourable estimates were obtained for all injury prevention measures except for stretching. Strength training reduced sports injuries to less than 1/3 and overuse injuries could be almost halved.” (7)
Following a 6-week hip abductor strengthening program, ITBS patients demonstrate a 35% to 50% increase in abductor muscle strength and were free of ITBS pain while running indicating a clear relationship between hip abductor muscle weakness, side-to-side imbalances in strength, and the development and effective treatment of ITBS. (4)
Biomechanics of ITBS suffers
The development of iliotibial band syndrome appears to be related to increased peak hip adduction and knee internal rotation. These combined motions may increase iliotibial band strain causing it to compress against the lateral femoral condyle. The data suggests that treatment interventions should focus on controlling these secondary plane movements through strengthening, stretching and neuromuscular re-education. (5)
Weakness of the hip abductor muscles may result in changes in running biomechanics which may necessitate greater passive restraint from the IT band while running and, over time, lead to the development of ITBS.
Strength Exercises for ITBS intervention
In this section we demonstrate many of ‘most effective’ – by measurement of isolation and activation forces – exercises you can do in your own home for the intervention of ITBS. Please ensure all care is taken to complete the exercises safely and correctly. Many detailed instructional videos for these exercises are available elsewhere online.
Strength training affects greatest adaptation when completed at higher-load, lower repetition(15). Reps of 6 or 7 approaching failure, in sets of 3-4 depending on experience and conditioning. We recommend you add resistance bands(12), weights or similar to the following exercises to facilitate this fatigue and ‘near-failure’. Rests between sets should be between 30-60 seconds(13).
While there are many hip abductor exercises, two ‘side-laying’ movements were shown to best isolate individual abductor muscles.
The side-lying hip-abduction exercise was the best exercise for activating the gluteus medius (10) with little activation of the tensor fascia latae and anterior hip flexors. (6)
Start sidelying on non-dominant side. Subject flex the hip and knee of the support side and then abduct the dominant leg to approximately 30 degrees while maintaining neutral or slight hip extension and knee extension with the toes pointed forward gradually up and down.
The ‘clam’ or ‘clam shell’ exercise resulted in the greatest activation of the anterior hip flexors with little activation of the gluteus medius and gluteus maximus. (6)
Start position is sidelying with hips flexed to approximately 45 degrees, knees flexed, and feet together. Externally rotate the top hip to bring the knees apart then slowly returns to start position.
For each of the major abductor muscle, the greatest two exercises for activation (by maximal voluntary muscle contraction)(10) are listed as follows,
Glute Medius
- Sideplank w/ Abduction
Start in a side plank. Keep shoulders, hips, knees, and ankles in line bilaterally, and then to rise to plank position with hips lifted off ground to achieve neutral alignment of trunk, hips, and knees. Allow upper extremity support. While balancing on elbows and feet, raise the top leg into abduction then lower leg. Maintain plank position throughout all repetitions
- Single Leg Squat
Stand on the dominant leg, slowly lowering the buttocks then extend back to standing.
Glute Maximus
-
- Front Plank w/ Hip Extension
Start prone on elbows in plank with trunk, hips, and knees in neutral alignment. Lift the dominant leg off of the ground, flexes the knee of the dominant leg, and extends the hip past neutral hip alignment by bringing the heel toward the ceiling then return to parallel.
- Gluteal Squeeze
In standing with feet shoulder-width apart, squeeze gluteal muscles then relax. Contract the gluteal musculature during the exercise.
- Front Plank w/ Hip Extension
Tensor Fasciae Latae
- Side Laying Hip Abduction
Start sidelying on non-dominant side. Flex the hip and knee of the support side and then abduct the dominant leg to approximately 30 degrees while maintaining neutral or slight hip extension and knee extension with the toes pointed forward slowly up and slowly down.
- Standing Hip Abduction w/ Resistance Band
While standing with weight balanced vertically over the dominant leg, abduct the unloaded leg laterally before returning to neutral.
Add a resistance band as required.
Prevention, Intervention or Improved Performance?
Abductor exercises are a good intervention for existing sufferers of ITBS. Strength training for injury prevention and performance should be specific to activity and relative to range of movement during anticipated running conditions. In hard hiked hills this may call for a strength programme of step-ups, squats or lunge-type exercises.
The exercises demonstrated above are focused around intervention of existing ITBS.
Foam Rolling for ITBS prevention and intervention
There is no evidence to support the activity of foam rolling to reduce onset or recovery of ITBS.
Foam rolling may help with Range of Movement (RoM) and Delayed Onset Muscle Soreness (DOMS) (8-9) – neither of which are related to ITBS. No link is made to foam rolling as remedial work for ITBS.
(1) A retrospective case-control analysis of 2002 running injuries Taunton JE et al (2002)
(2) Iliotibial band syndrome in runners: innovations in treatment Fredericson M et al (2005)
(3) Hip abductor weakness in distance runners with iliotibial band syndrome Fredericson M et al (2000)
(4) Hip muscle weakness and overuse injuries in recreational runners Niemuth PE et al (2005)
(5) ASB clinical biomechanics award winner 2006 prospective study of the biomechanical factors associated with iliotibial band syndrome Noehren B et al (2007)
(6) Hip Muscle Activity During 3 Side-Lying Hip-Strengthening Exercises in Distance Runners Joseph M. McBeth et al (2012)
(7) The effectiveness of exercise interventions to prevent sports injuries: a systematic review and meta-analysis of randomised controlled trials Jeppe Bo Lauersen et al (2013)
(8) Foam Rolling for Delayed-Onset Muscle Soreness and Recovery of Dynamic Performance Measures Gregory E. P. Pearcey et al (2015)
(9) The effects of self‐myofascial release using a foam roll or roller massager on joint range of motion, muscle recovery, and performance: a systematic review Scott W. Cheatham et al (2015)
(10) Gluteal muscle activation during common therapeutic exercises Distefano LJ et al (2009)
(11) Electromyographic Analysis Of Gluteus Medius And Gluteus Maximus During Rehabilitation Exercises K Boren et al (2011)
(12) Strengthening exercises performed with elastic tubing seem to be an efficient resistance exercise and a feasible and practical alternative to traditional resistance equipment. Sundstrup E (2012)
(13) Rest interval between sets in strength training de Salles BF (2009)
(14) Effects of Low- vs. High-Load Resistance Training on Muscle Strength and Hypertrophy in Well-Trained Men. Schoenfeld BJ (2015)